



GERD / Acidity / Acid Reflux
AIC’s GERD, Acidity, Acid Reflux Wellness bundle targets the root causes of GERD and Acidity, providing FAST and LASTING relief from heartburn, bloating, and discomfort. This bundle combines clinically-proven ingredients to address low stomach acid, reduce inflammation, enhance digestive enzymes, and promote a healthy gut microbiome.
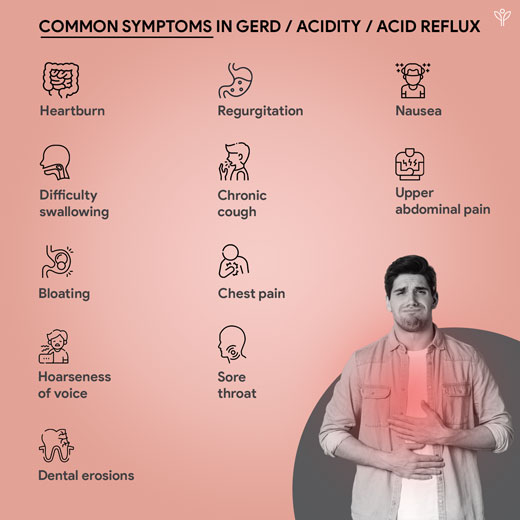
Understanding GERD / Acidity / Acid Reflux
Gastro Esophageal Reflux Disease (GERD) – also referred to as acid reflux or ‘heartburn’ is a chronic digestive condition characterized by the backflow of stomach contents into the esophagus, often leading to a range of unpleasant symptoms such as heartburn, regurgitation, and difficulty swallowing.
It affects approximately 11.0%-29.2% of the population worldwide and can significantly impair an individual’s quality of life. (Cho et al., 2013) In India, the prevalence of GERD is estimated to be around 7.6%-30 % (Bhatia et al., 2019).
What we have in GERD / Acidity / Acid Reflux



Reference
Bhatia, S., Makharia, G., Abraham, P., Bhat, N., Kumar, A., Reddy, D. N., Ghoshal, U. C., Ahuja, V., Rao, G. V., Devadas, K., Dutta, A. K., Jain, A., Kedia, S., Dama, R., Kalapala, R., Alvares, J. F., Dadhich, S., Dixit, V. K., Goenka, M. K., … Wadhwa, R. T. (2019). Indian consensus on gastroesophageal reflux disease in adults: A position statement of the Indian Society of Gastroenterology. In Indian Journal of Gastroenterology (Vol. 38, Issue 5, p. 411). Springer Science+Business Media.
Cho, J., Ahn, Y., Lee, D., & Son, C. (2013). Distributions of Sasang constitutions and six syndromes in patients with functional dyspepsia and healthy subjects. In Deleted Journal (Vol. 33, Issue 5, p. 626).
Dirac, M. A., Safiri, S., Tsoi, D., Adedoyin, R. A., Afshin, A., Akhlaghi, N., Alahdab, F., Almulhim, A. M., Mini, G., Ausloos, F., Bacha, U., Banach, M., Bhagavathula, A. S., Bijani, A., Biondi, A., Borzì, A. M., Colombara, D. V., Corey, K. E., Dagnew, B., … Veisani, Y. (2020). The global, regional, and national burden of gastro-oesophageal reflux disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. In The Lancet. Gastroenterology & hepatology (Vol. 5, Issue 6, p. 561). Elsevier BV.
Gaddam, S., & Sharma, P. (2011). Shedding light on the epidemiology of gastroesophageal reflux disease in India—a big step forward. In Indian Journal of Gastroenterology (Vol. 30, Issue 3, p. 105). Springer Science+Business Media.
Hernández-Mondragón, O. V., Mottú, R. A. Z., Contreras, L. F. G., Aguilar, R. A. G., Solórzano-Pineda, O. M., Blanco‐Velasco, G., & Pérez, E. M. (2020). Clinical feasibility of a new antireflux ablation therapy on gastroesophageal reflux disease (with video). In Gastrointestinal Endoscopy (Vol. 92, Issue 6, p. 1190). Elsevier BV.
Jones, R. C., Junghard, O., Dent, J., Vakil, N., Halling, K., Wernersson, B., & Lind, T. (2009). Development of the GerdQ, a tool for the diagnosis and management of gastro‐oesophageal reflux disease in primary care. In Alimentary Pharmacology & Therapeutics (Vol. 30, Issue 10, p. 1030). Wiley.
Jones, R., Coyne, K. S., & Wiklund, I. (2007). The Gastro‐oesophageal Reflux Disease Impact Scale: a patient management tool for primary care. In Alimentary Pharmacology & Therapeutics (Vol. 25, Issue 12, p. 1451). Wiley.
Katz, P. O., Dunbar, K. B., Schnoll‐Sussman, F., Greer, K. B., Yadlapati, R., & Spechler, S. J. (2021). ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease [Review of ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease]. The American Journal of Gastroenterology, 117(1), 27. Lippincott Williams & Wilkins.
Kim, M. J., Schroeder, S. E., Chan, S., Hickerson, K., & Lee, Y. (2022). Reviewing the User-Centered Design Process for a Comprehensive Gastroesophageal Reflux Disease (GERD) App. In International Journal of Environmental Research and Public Health (Vol. 19, Issue 3, p. 1128). Multidisciplinary Digital Publishing Institute.
Wang, X., Wright, Z., Patton-Tackett, E., & Song, G. (2023). The Relationship between Gastroesophageal Reflux Disease and Chronic Kidney Disease. In Journal of Personalized Medicine (Vol. 13, Issue 5, p. 827). Multidisciplinary Digital Publishing Institute.
